



Oh What a Vault!

If any of you are like me, you are already feeling withdrawl symptoms now that the Olympics are over. My whole family loves to crowd around the TV once every 4 years to watch new Olympians become our heroes. Did anyone see McKayla Maroney do the vault? She skied to unbelievable heights with incredible precision, and the vault she did during qualifiers in particular was one of the most memorable moments of these Olympic Games with my family.
Now that the Olympics are over, and we are back in the office, vaulting takes on a new revelance. Many refractive surgeons now believe that for those who qualify, ICL’s are one of the most exciting procedures available in refractive surgery today. I believe in the procedure enough that we selected it for my wife, Heather, even though she was a LASIK candidate. One of the most important aspects of excellent ICL surgery is of course… Drum Roll… Vault!
In this first edition of the newly created Parkhurst blog, I’d like to review some of the important aspects of ICL vault.
The ICL is available in 4 sizes. Many times, we are left to choose between 2 sizes, when in a perfect world, there was an in-between size that we could select for a particular eye. The ICL is of course an implantable lens made of collagen copolymer that is implanted in the ciliary sulcus of the phakic eye to treat myopia. In the FDA trial, Staar got approval for sizing of the ICL by using the horizontal white-to-white measurement as a close approximation to ciliary sulcus diameter. If an ICL is too long relative to the diameter of the sulcus, vaulting increases. Contrariwise, if an ICL is too short relative to the sulcus diameter, vaulting decreases.
Adequate vault is very important in eyes implanted with ICLs because we know that overvaulting may cause crowding of the angle and the potential risk for IOP elevation. On the other hand, inadequate vault increases the risk of anterior subcapsular opacification. We want vault that is just right.
Below are a few slit lamp photographs of what we look for and try to document on every post-op ICL chart.
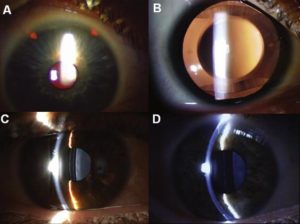
As you can see in slide A, the PI’s at 11 and 1 are very easy to see on retro-illumination. This photo is representative of how I make almost all of my PI’s. They are about 1.5 mm in diameter, very far out, placed at 11 and 1 under the lid. I intentionally try to hide them far out like this in order to decrease the incidence of dysphotopsias from the PI. Ideally, they can be seen by normal slit inspection because this is the best way to confirm patency. However, sometimes, PI’s may only be visible by retro-illumination if pannus overrides and gets in the way. Note: it is possible for a PI to retroilluminate that is not patent.
Slide C and D demonstrate what I’ve found to be the best technique to judge and therefore document ICL vault. The narrow slit beam is directed an approximate 45 degree angle toward the center of the pupil. The slit beam traveling through the cornea is used as a reference landmark in order to judge the dark space between the ICL and the crystalline lens. If a patient has a normal 550 micron cornea, a 100% corneal thickness vault would approximate 550 microns. Some refractive surgery consultants will document vault in microns. Others document vault relative to central cornea thickness (CCT) e.g. vault = 150% CCT. In the setting of monocular surgery, having this information will allow us to most precisely select the perfectly sized ICL for the 2nd eye based on the vault achieved in the first eye. In most eyes (depending on AC depth), the ideal vault is between 250-850 microns. Furthermore, documenting vault will allow future comparison that may help in the differential diagnosis of rare perioperative complications such as iridotomy occlusion with pupil block IOP elevation.
The way I would document in my chart photograph C would be: lids clear, conj quiet, cornea clear, no wound leak, AC trace cells, Iris PI patent, ICL in the sulcus with 50% CCT vault, crystalline lens clear. As you can see, this ICL is slightly undervaulted.
The way I document in my chart the findings in photograph D would be: lids clear, conj quiet, cornea clear, no wound leak, AC slightly shallow and quiet, Iris PI patent, ICL in sulcus with 200% CCT vault, crystalline lens clear. As you can see, this ICL is slightly overvaulted.
Neither of these ICL’s should be exchanged so long as IOP is controlled. However, you can start to see the sweet spot for ICL vaulting. These would be at the lower and upper ranges of acceptable.
Next up: what some believe is an even better way to select ICL sizing… Ultrasound Biomicroscopy to measure the exact diameter of the ciliary sulcus.

If we are able to achieve perfect vaults in all eyes, we’ll have the judges looking like this!
Images:
1. Copyright (c) Tumbler, Inc.
2. Copyright (c) 2012 Bleacher Report, Inc. Turner Broadcasting System, Inc. All Rights Reserved. BleacherReport.com is part of Turner Sports Digital, part of the Turner Sports & Entertainment Digital Network. Certain photos copyright (c) 2012 by Getty Images.
3. Journal of Cataract & Refractive Surgery, Volume 36, Issue, 11, Pages 1976-1993, November 2010. Copyright (c) 2012 Elsevier Inc. All rights reserved.
4. (c) Copyright 2012 – Busted Coverage Sports . All Rights Reserved. Powered by WordPress Themes
